 German (DE)
German (DE)  English (US)
English (US)  Spanish (ES)
Spanish (ES)  French (FR)
French (FR)  Hindi (IN)
Hindi (IN)  Italian (IT)
Italian (IT)  Russian (RU)
Russian (RU) In June 1981, I was a young pulmonary fellow at one of the three Los Angeles hospitals where the first five cases of an unusual pneumonia in previously healthy young men were being identified. I read about them, as my colleagues did, in the Morbidity and Mortality Weekly Report (MMWR) – the small, dense bulletin the Centers for Disease Control had been publishing every week since 1952.
None of us yet knew what we were seeing. What MMWR gave us was a signal early enough to act on, and a system trustworthy enough that we did. What became Aids would, over the next decade, reshape every assumption I held about clinical medicine. I have spent the 40 years since then practicing critical care at UCLA, and the federal scientific architecture that produced that signal in 1981 has been the bedrock of my work.
That architecture is being dismantled. On Friday, the presidential personnel office sent termination notices to members of the National Science Board, the body Congress created in 1950 to insulate the country’s basic-science funding from political pressure.
The dismissals came in brief emails, with no explanation. They are the latest in a year of changes that share a single design: the federal institutions American physicians depend on still exist, but the layer of independence inside each of them has been removed. The agencies remain on the page. They are no longer the agencies that gave me, in June 1981, a signal I could act on.
The pattern is procedural, and it is built around statutes Congress wrote to make this kind of capture difficult. Federal law requires advisory panels to be balanced in their viewpoints. It requires agencies to give reasoned explanations before changing longstanding rules. It ties federal vaccine coverage, by name, to recommendations from a specific advisory body.
Each of those rules presumed that political appointees would not simply walk around the bodies the law named. That presumption is no longer safe.
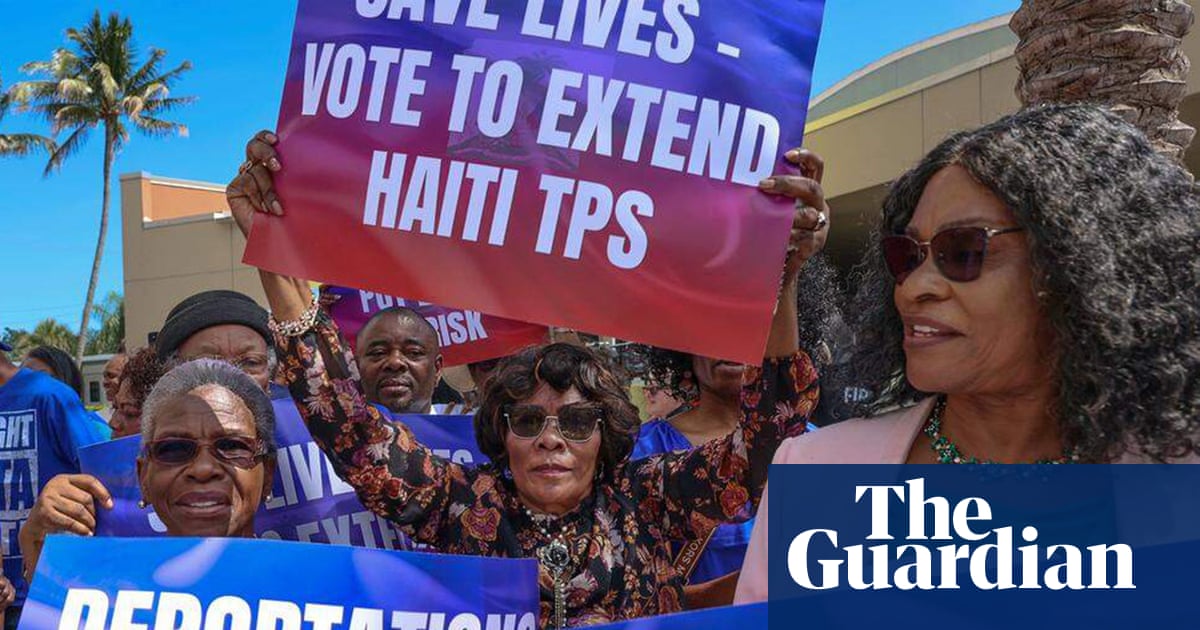
Last June, the secretary of health and human services dismissed all 17 members of the advisory committee on immunization practices, the panel that for 60 years has determined which vaccines pediatricians offer and insurers cover without copay. By January, the federal childhood vaccine schedule had been cut from 17 recommended diseases to 11, without any involvement from the committee.
In March, a federal judge stayed those decisions, finding that “even under the most generous reading”, only six of the 15 replacement members had any meaningful expertise in vaccines. This month, the committee’s charter was rewritten to add a focus on vaccine “harm”. The committee is still meeting. Its independence is gone.
The same pattern reached the data physicians rely on. An audit in the Annals of Internal Medicine in January documented that 38 of the CDC’s 82 routinely updated public surveillance databases have stopped publishing without explanation – and that 87% of those paused databases concerned vaccination.
Last week, MMWR – the journal that on 5 June 1981, published those first five cases of what would become Aids – rejected a peer-reviewed paper on Covid-19 vaccine effectiveness after it had cleared scientific review and been scheduled for publication.
The acting CDC director objected to a methodology, the test-negative design, that MMWR itself had used in a flu-vaccine paper a week earlier. A clinician relying on either system today is relying on something that has been edited by political preference rather than by scientific judgment.
And on Friday, the pattern reached the basic science that produces tomorrow’s medicine. The National Science Board oversees the National Science Foundation’s $9bn in annual research grants. Its members serve six-year staggered terms, by statute, so that no single president can replace them at once. The basic research the foundation approves becomes, a decade or two later, the imaging machines that diagnose cancer and the gene-editing tools that treat it.
The board’s decisions this April shape what physicians can offer patients in 2040. Friday’s firing caps a year of erosion at the agency, which has had no permanent director since April 2025 and whose budget the administration has proposed cutting by more than half.
The decisions I make at the bedside still get made. They simply get made with more guesswork. The antibiotic I choose for a patient in septic shock now relies on resistance patterns (surveillance data showing which antibiotics still kill which bacteria in a given hospital, region, or country) that, in some cases, are no longer being published.
The booster I counsel for a transplant patient is recommended based on a CDC analysis the agency’s leadership rejected this month. The young father who asks me whether the new pediatric vaccine schedule means his daughter is at greater risk than her older brother was is asking a question I would once have answered without hesitation.
The signal that came from MMWR in June 1981 reached the bedside because the systems behind it were trustworthy: independent panels, transparent surveillance, editorial firewalls, staggered terms designed to outlast any single administration. None of that was an accident. It was built deliberately, over decades, by people who understood that public health information has to be insulated from the people in power if it is going to be believed by the public it serves.
That insulation is what is being removed. The agencies will continue to exist. They will issue recommendations and publish journals and approve research grants. But the work they produce will increasingly be shaped by what political appointees prefer the public to know, rather than by what the public needs to know.
A country that still has the agencies but no longer has their independence has lost something more difficult to rebuild than any institution: the earned confidence, accumulated over generations, that when the system tells you something, the system is telling you the truth.
-
Robert B Shpiner, MD, FCCP, FAASM, is a clinical professor of medicine (pulmonary and critical care) at the David Geffen School of Medicine at UCLA, where he has practiced critical care for more than 40 years. He was a pulmonary fellow at one of the three Los Angeles hospitals in which the first five MMWR-reported cases of what would become Aids were identified in June 1981





















Comments